SuNMaP 2
SUPPORT TO
NIGERIA'S NATIONAL MALARIA PROGRAMME
2018-2021
End of programme summary


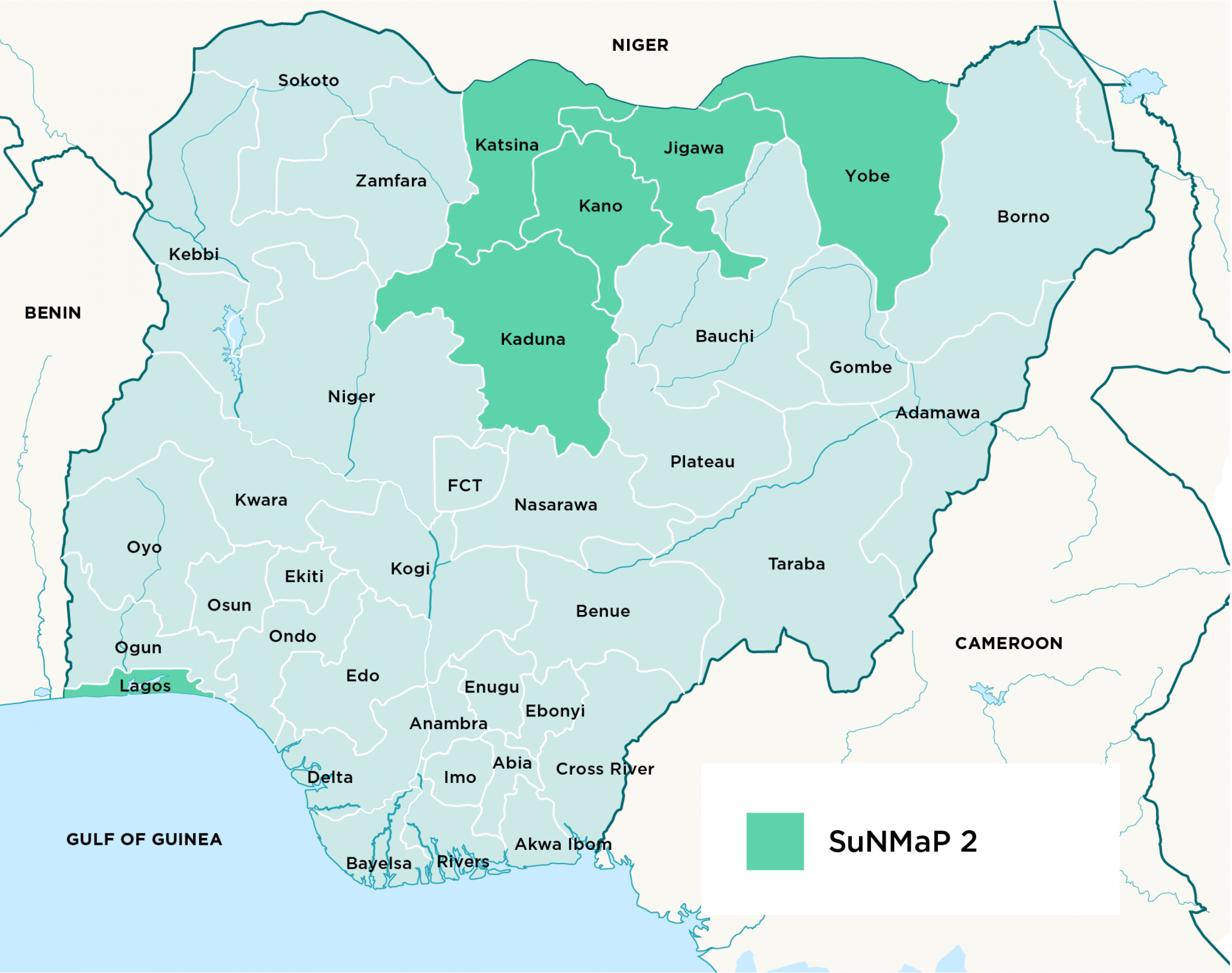
The Support to Nigeria's National Malaria Programme (SuNMaP 2), operational since 2018, was a UK aid-funded programme designed to support national government efforts to further reduce Nigeria’s malaria burden. SuNMaP 2 followed on from the predecessor programme, SuNMaP, that was also led by Malaria Consortium and ran from 2008-2016.
SuNMaP 2 had a focus on integrating malaria prevention and treatment, as well as other interventions, at the community and service delivery levels through public and private sector partnerships. Improving the planning, financing and delivery of sustainable malaria programmes across 165 local government areas in six states of Nigeria: Jigawa, Kaduna, Kano, Katsina, Lagos and Yobe was a primary objective.
Ensuring government involvement and stewardship of SuNMaP 2 was an integral component to ensure that the interventions were sustainable. Malaria Consortium and its partners worked in collaboration with government structures at the national and sub-national levels to coordinate and harmonise the planning, implementation and evaluation of programme interventions.
Due to the UK Government’s decision to cut their Overseas Development Assistance budget, SuNMaP 2 activities were ceased with almost immediate effect three years before the programme’s planned end. Despite this premature curtailment, the programme achieved a number of key results.
Programme goals
Across the six supported states, SuNMaP 2's overall goal for the original five-year programme was to support a fall in malaria morbidity in the supported states and falling levels of all causes of mortality in children under five, in the supported states during the span of the programme.
Within these overall goals were five key outputs:
- Strengthened government stewardship at national level and in SuNMaP 2 supported states
- More efficient and equitable malaria prevention and treatment services delivery
- Increasing the sustainable availability of antimalarial commodities
- Helping citizens and institutions to better engage with Nigeria's malaria response
- Embedding an evidence-based learning environment within the National Malaria Elimination Programme (NMEP) and state-level Malaria Elimination Programmes (SMEPs).

Key achievement 1
Strengthened government stewardship at national level and in SuNMaP 2 supported states
As part of programme activities to strengthen government stewardship and grow institutional capacity for malaria programming at national and state levels, the programme made remarkable progress in achieving results in domestic resource mobilisation. With the increased need to propel sustainable solutions for health programmes (independent of donor support), the SuNMaP 2 initiatives resulted in increased budgetary allocation for malaria in programme locations including at the national level and in four supported states: Kano, Yobe, Kaduna and Lagos.

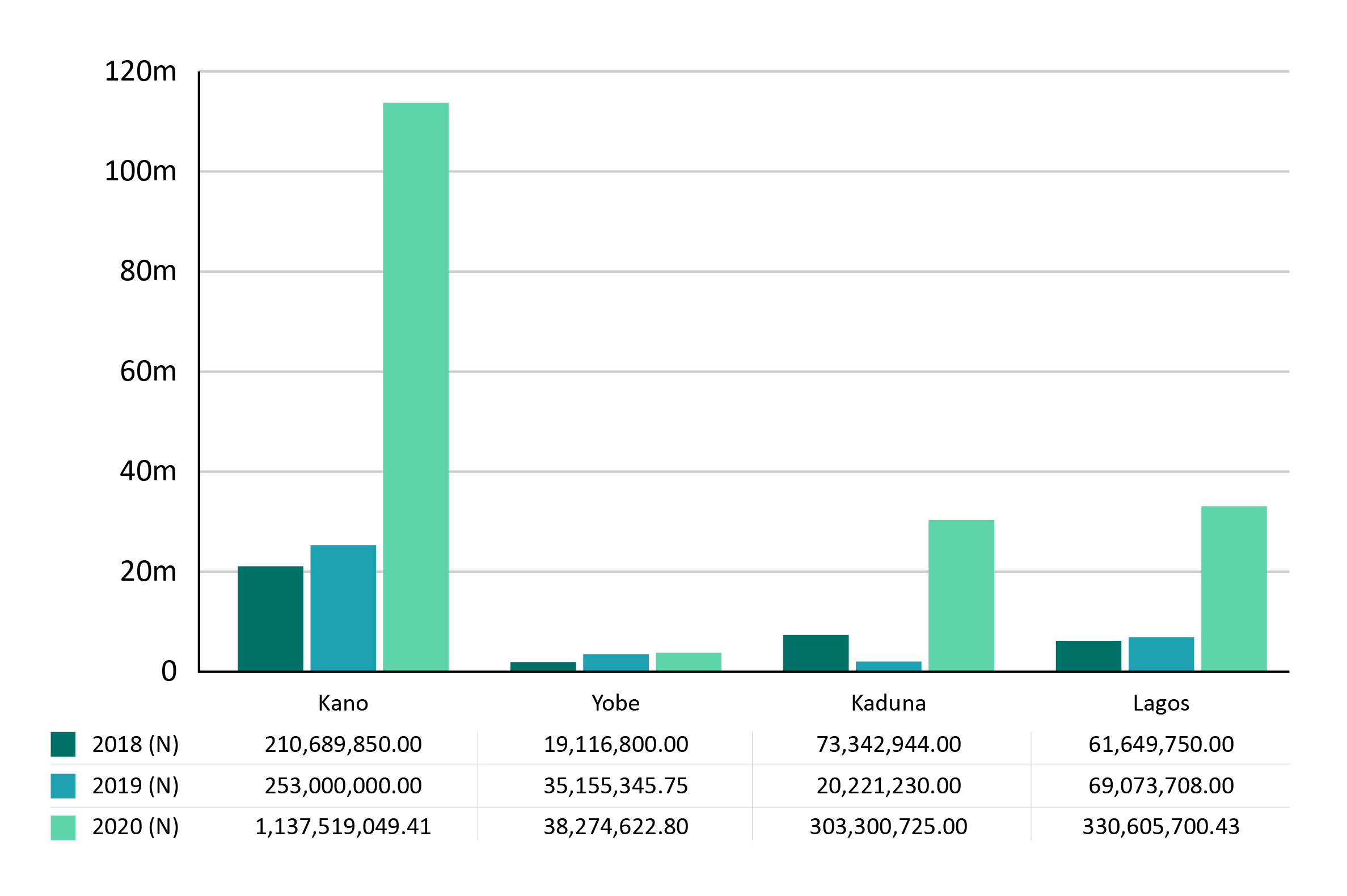
Proportion of total annual malaria expenditure from domestic sources in Kano, Yobe, Kaduna and Lagos states, 2018-2020
Proportion of total annual malaria expenditure from domestic sources in Kano, Yobe, Kaduna and Lagos states, 2018-2020
Key achievements in this area include:
- The introduction and roll out of an 18-month rolling plan for the malaria programme at national and state levels
- Development of systems for malaria expenditure tracking
- Capacity building at the national level and particularly in the six supported states to develop yearly financial plans
- Political economy analysis and fiscal space assessment studies to improve domestic resource allocation to the malaria programme
- Technical assistance to support the development of the 2019 Malaria Programme Review (MPR) and the inclusion of Value for Money (VfM) in programme management integration in the new National Malaria Strategic Plan (2021-2025)
- Technical assistance to the NMEP on the development of coordination framework, capacity building framework and resource mobilisation framework.
Impact of programme closure in this area
The full implementation of the 18-month rolling plan may not be achieved due to the early closure of the programme. This will affect the development of yearly financial plans and the inclusion of malaria programme needs in government budgets at the executive and legislature levels.
The integration of the planning process with the budgeting cycle and utilisation of lessons learnt across all programme locations will be impacted by the early closure of the programme.
Key achievement 2
Increasing the sustainable availability of antimalarial commodities
In order to improve commodity management and reduce stockout rates for malaria commodities in supported states, SuNMaP 2 undertook a number of activities to improve supply change management including:
- Partnership with the Global Fund (GF) on implementation of the National Supply Chain Integrated Project (NSCIP) blueprint
- Technical assistance to Logistic Coordination Management Unit for integrated reporting
- Training for supply chain management stakeholders on quantification reviews
- Review of state supply chain management plans
- Review of multi-year National Malaria Health Product quantification and forecast
- End to end malaria commodity audit in all six states
- Provision of limited quantities of malaria commodities
- Supported states to identify and calculate the most effective channel for LLIN distribution through the use of the NetCALC tool
- Continuous long-lasting insecticidal net (LLIN) distribution through antenatal care and schools
- Supported the revision of the integrated vector management decision tree to provide guidance for the targeting of malaria intervention according to local needs.

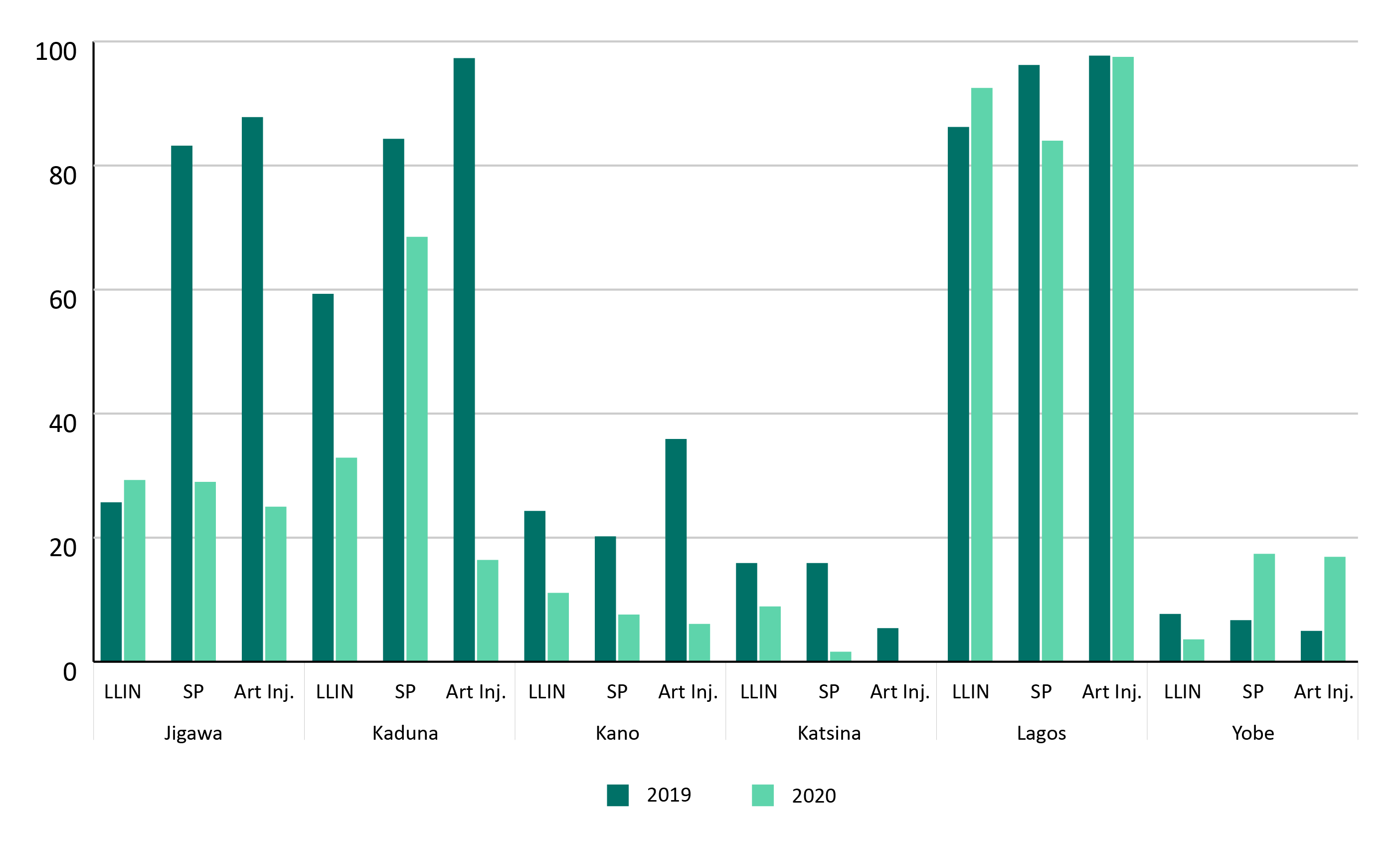
Percentage of health facilities that experienced stock-outs of malaria commodities in SuNMaP2-supported states in 2019 and 2020.
Percentage of health facilities that experienced stock-outs of malaria commodities in SuNMaP2-supported states in 2019 and 2020.
As seen in the graph, there was an overall reduction in stock-outs of malaria commodities in four of the supported states in 2020 compared with corresponding rates in 2019. In states where reduction targets were not met, including in Lagos, problems were attributed to the winding down of national procurement of some commodities and protraction in government supplies.
Informed by previous experience of private sector engagement in Nigeria, particularly as a part of the predecessor SuNMaP, the SuNMaP 2 team also formed a workstream focusing on market systems development in order to facilitate an unprecedented level of public-private dialogue and coordination in the fight against malaria in Nigeria.
The core aim for the market systems development workstream was to facilitate the development of sustainable markets for malaria commodities and increase advocacy to the Nigerian government and public on the security of these commodities, particularly of LLINs.

Key achievements in the workstream were:
- Artemisinin Combination Therapy (ACT) and malaria Rapid Diagnostic Tests (mRDTs) co-payment transition plan developed to guide the availability of quality-assured and affordable case management commodities in the private health care sector - 51 percent of this plan was completed by March 2021
- Supporting the NMEP to develop strategic and operational processes in order to achieve set objectives including streamlining market systems plans into the Malaria Operational Plans (MoPs)
- Mapping of key commercial outlets and landscape assessment for ACTs, mRDTs and LLINs to inform implementation strategies, such as coordinating engagements between NMEP and other relevant stakeholders
- Supported the NMEP to undertake a landscape assessment for PPPP (Public Private Philanthropy Partnership) and creation of a PPPP subcommittee, linked to the existing Programme Management subcommittee of NMEP to ensure private and philanthropic stakeholders efforts are well coordinated with that of their public counterpart as part of the overall coordination by the NMEP
- Collaboration with the National Agency for Food and Drug Administration and Control for routine market monitoring
Impact of programme closure in this area
The early closure of SuNMaP2 affected the programme’s anticipated support in developing a procurement plan for malaria commodities in Year 3 and transitioning to government funding for the procurement of malaria commodities in line with the broader sustainability goal of the programme.
Key achievement 3
Improving overall malaria service delivery
Community-based service delivery, seasonal malaria chemoprevention, severe malaria case management
Community-based service delivery
SuNMaP 2 supported efforts to institutionalise the Community Health Influencer Promoters and Service (CHIPS), a government-led initiative, as a sustainable approach to the delivery of community-based health services. This included the introduction of the CHIPS programme in 10 local government areas (LGAs) in Kano state, reaching a total of 58,523 children under five.
SuNMaP 2 also supported training for over 1,800 CHIPS, 187 CHIPS supervisors and 214 community engagement focal persons in Kano state. This was commended by stakeholders for its impact on strengthening community-based targeted interventions for malaria case management and the perceived resultant effect on reducing mortality due to malaria, particularly amongst vulnerable groups and those in hard-to-reach communities.
More than 90 percent of children under-five with confirmed malaria were treated with ACTs.
Other key approaches for SuNMaP 2's work with the CHIPS programme include:
- Harmonisation of existing iCCM activities with new CHIPS activities
- Resource mobilisation including government sources
- Capacity building of CHIPS agents and CHIPS supervisors (training, clinical mentoring and supportive supervision)
- Provision of CHIPS commodities, data collection tools and personal protective equipment (PPE)
- Establishment of a system for performance assessments
- Dissemination of CHIPS programme learning (phase 1) and planning for scale-up (phase 2 and phase 3)
The work undertaken to support CHIPS took on greater importance in 2020 in the face of the COVID-19 pandemic as a shift from larger public health facilities to community-based services was necessitated by COVID-19 control measures enacted by the government.


Capacity building for service delivery
SuNMaP 2 also underpinned improvements in community-based service delivery with capacity-building activities at state and national levels. Key approaches in this area included:
- Capacity building plan/quality assurance (QA) framework at national and state levels
- Capacity building of service providers on malaria in pregnancy (MiP) and case management of uncomplicated malaria
- Supportive supervision using on-the-job capacity building (OJCB), mentoring and competency assessment tools
- Collaboration with the Global Fund on instituting external quality assurance (EQA) on the microscopic diagnosis of malaria
Key achievements included:
- 3,976 service providers trained on MiP and case management of uncomplicated malaria
- 48 percent adherence to standards in MiP and case management of uncomplicated malaria
- The mean malaria microscopy EQA performance of health facilities ranged from 49 percent in Kano to 76 percent in Kaduna (Jan-March 2021).


MiP training at Aminu Kano Teaching Hospital, November 2020
MiP training at Aminu Kano Teaching Hospital, November 2020
SuNMaP 2 also oversaw the distribution of seasonal malaria chemoprevention (SMC) in Jigawa state in collaboration with Malaria Consortium's wider SMC programme.
92 percent and 95 percent of all eligible children received SMC interventions in Jigawa state in 2020 and 2019, respectively (SMC survey coverage reports 2020 and 2019).

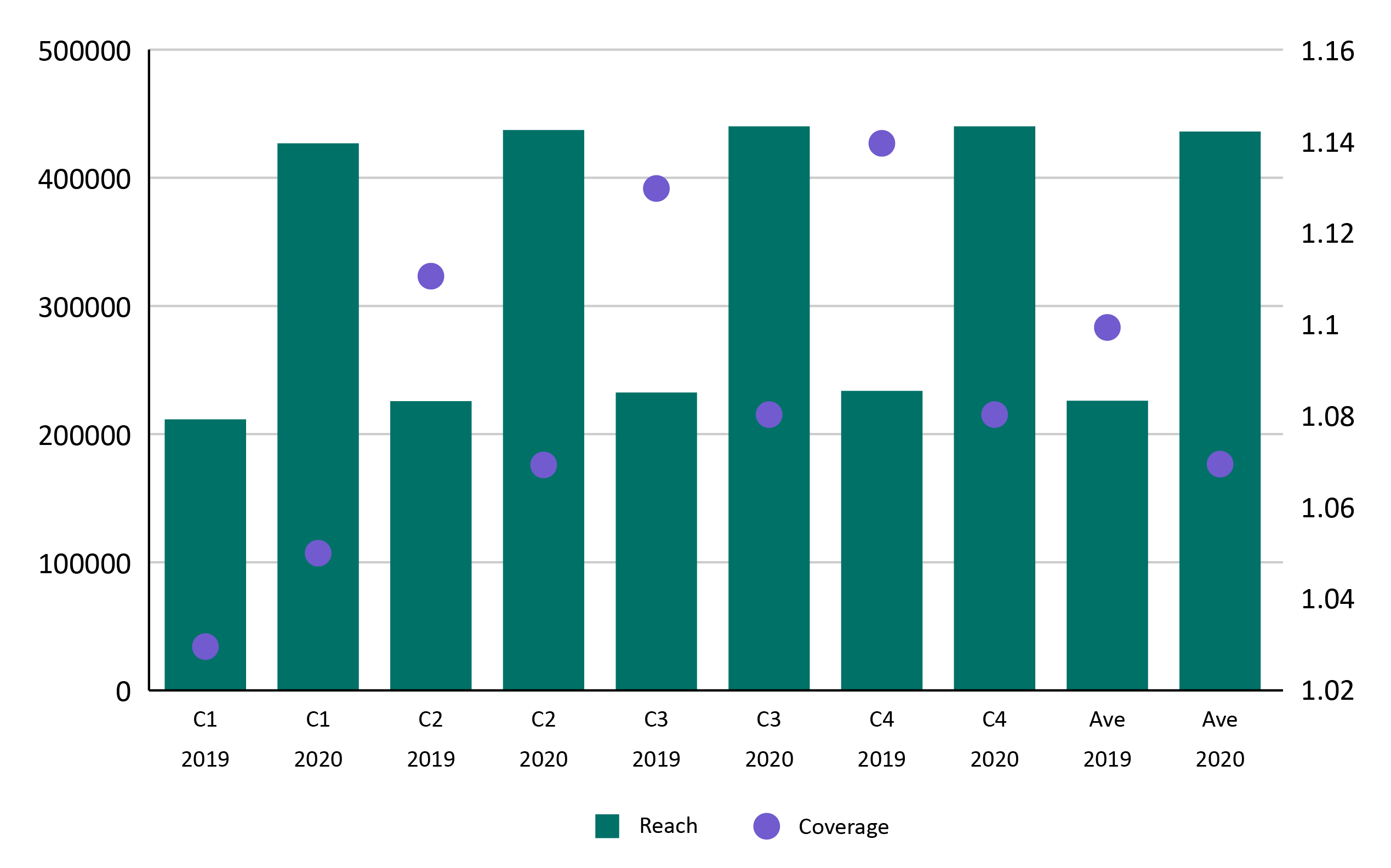
Administrative SMC coverage by cycle (c) and year in Jigawa state
Administrative SMC coverage by cycle (c) and year in Jigawa state
On average, a total of 436,077 and 226,045 eligible children received SMC in Jigawa state in 2020 and 2019, respectively (SMC administrative coverage reports, 2020 and 2019).
Following the closure of SuNMaP 2, SMC implementation in Jigawa state was successfully transitioned to Global Fund funding under the New Funding Model (NFM) grant (2021-2023).


Key SMC approaches included:
- Supply chain management including procurement of Sulfadoxine-Pyrimethamine + Amodiaquine (SPAQ)
- Selection and capacity building of personnel (training and supervision)
- Social behaviour change communication (SBCC) initiatives to support confidence in the intervention
- Door-to-door distribution of SPAQ
- Enhanced COVID-19 safety measures in alignment with normative guidance from the RBM Partnership to End Malaria
- Monitoring and evaluation and pharmacovigilance.
Severe malaria case management
Severe malaria case management refers to the handling of cases where malaria becomes complicated and the patient is affected by organ failure and/or other abnormalities in blood or metabolism.

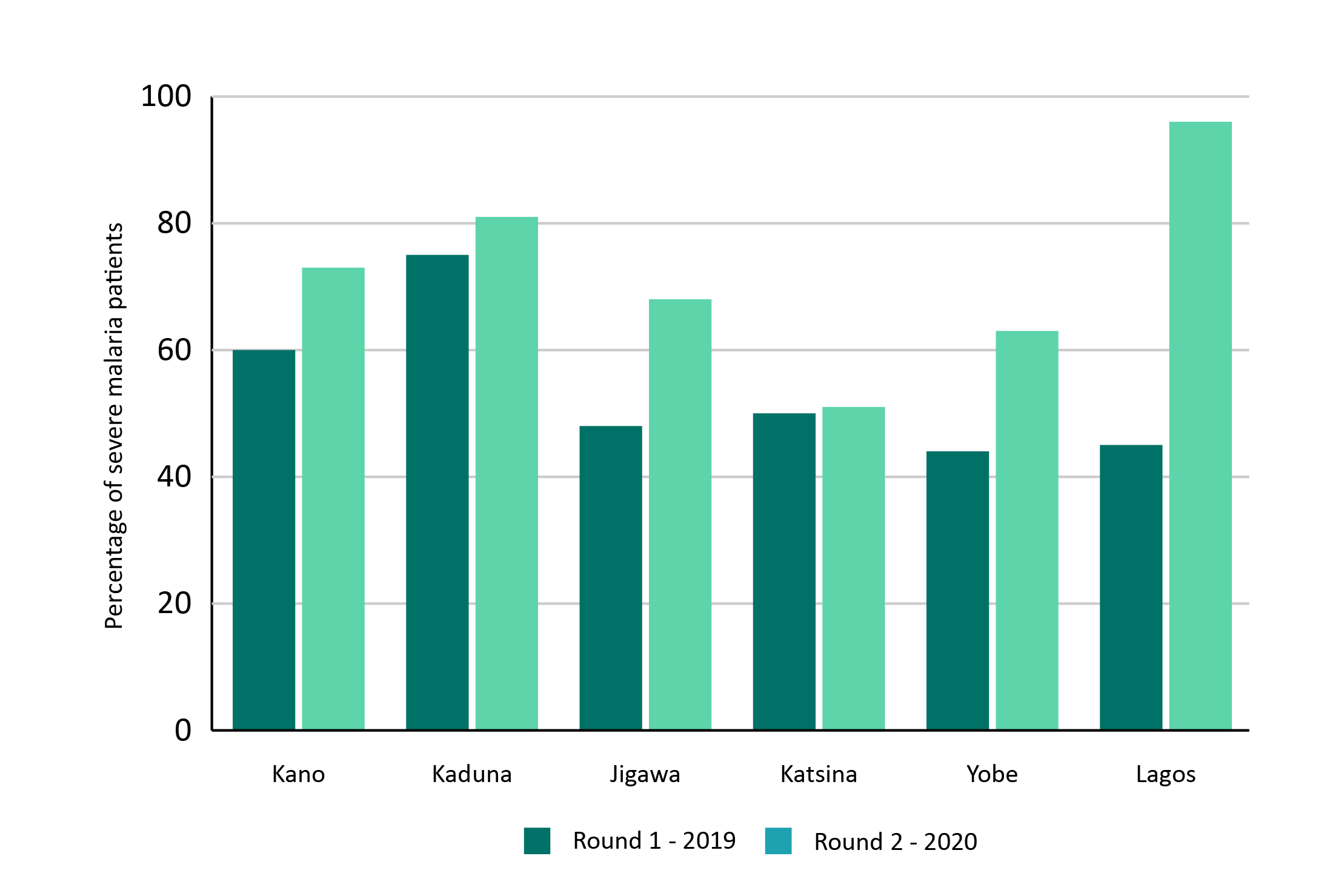
Artesunate treatment rates for severe malaria admission in 62 secondary and tertiary hospitals in SuNMaP2 supported states, 2019 and 2020
Artesunate treatment rates for severe malaria admission in 62 secondary and tertiary hospitals in SuNMaP2 supported states, 2019 and 2020
SuNMaP 2 oversaw increases in the use of artesunate for severe malaria case management through a range of methods, including:
- Continuous quality improvement (QI) cycles consisting of annual hospital assessments, enhanced feedback delivery, creation of hospital QI teams and post‐assessment supportive follow‐up visits
- Capacity building of service providers on severe malaria case management
- Provision of limited quantities of injectable artesunate
- Distribution of national malaria case management guidelines and job aids.


In addition to the distribution of SMC in Jigawa state, SuNMaP 2 distributed malaria prevention, diagnostic and treatment commodities to health facilities across the six supported states to further support malaria service delivery.
Further to the procurement and distribution of malaria commodities, the SuNMaP 2 team also facilitated dialogues between citizens and decision-makers at a local and state level to improve accountability for malaria funding and increase local ownership of the work.
35,577 deaths were averted
Figure estimated using the Lives Saved Tool (LiST) methodology and analysis.
The cost-effectiveness of the programme, as measured in terms of cost per death averted for LLIN, mRDT and ACT are £19.70, £526.40 and £38, respectively. Whereas the cost per disability-adjusted life year (DALY) averted for LLIN, mRDT and ACT are £0.64, £16.98 and £1.23, respectively. The programme’s performance on cost-effectiveness metrics is in line with international benchmarks and also broadly comparable to SuNMaP. This VFM analysis shows that the implementation of malaria interventions by SuNMaP2 across the six supported states was cost-effective.
IN NUMBERS:
Malaria commodities distributed by SuNMaP 2
549,712 LLINs to protect their users from mosquitoes for up to three years
518,432 rapid diagnostic tests (mRDTs) to support the quick diagnosis and treatment of malaria
120,660 doses of artemisinin-based combination therapy (ACT) to treat cases of P. falciparum malaria
Impact of programme closure in this area
Quality of care in inpatient malaria case management including the use of artesunate for severe malaria will be affected as SuNMaP 2 has been the only programme implementing the innovative approach dubbed continuous QI cycles in the six supported states. This is particularly important in the context of COVID-19 since delayed treatment seeking to health facilities and referrals could result in more severely ill cases coming to health facilities.
The roll-out of CHIPS in Kano and Kaduna was still in the early stages of implementation. With the closure of SuNMaP 2, there is a need for the government to increase its funding or another donor to support the ongoing roll-out as well as scaling up to additional LGAs in Kano and Kaduna states.
Key achievement 4
Better informed citizens and institutions
Informed citizens and institutions who are engaged in the fight against malaria at all levels are crucial to the success and sustainability of interventions. On this basis, SuNMaP 2 has worked to reach these groups (across the supported states and at a national level), to engage with malaria messages.
Some of the key approaches used to achieve this included:
- Formative research on the underlying causes of the gap between awareness and use of malaria commodities
- Malaria/COVID-19 communication strategy
- Community feedback loop
- Community score card
- Advocacy for increased malaria funding through town hall meetings and state policy dialogues (see case study).
Key achievements include:
- Improvements in the proportion of women between the age of 15 and 49 in the lowest wealth quantile who reported seeing or hearing a malaria message in the past six months [46 percent vs 30 percent] (Omnibus survey, February 2020)
- 130 community coalitions (CCs) on malaria established in five programme states
- 853 Ward Development Committees (WDCs) and Facility Health Committees (FHCs) trained on malaria prevention and treatment.

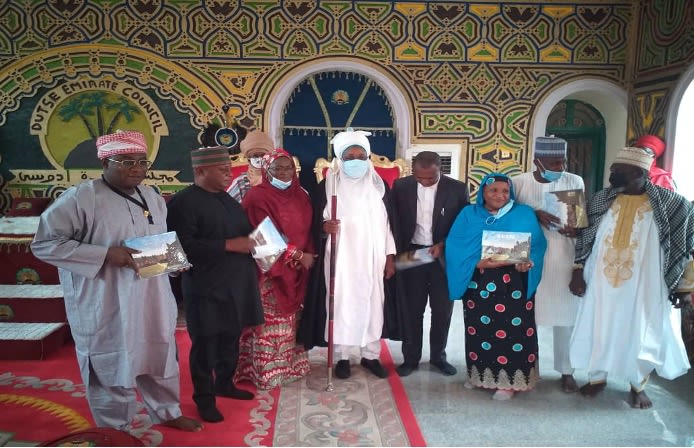
Advocacy visit to the Emir of Dutse Jigawa State, HRH Alhaji Nuhu Sanusi
Advocacy visit to the Emir of Dutse Jigawa State, HRH Alhaji Nuhu Sanusi
CASE STUDY: New town hall meetings in Nigeria lead to concrete commitments on malaria funding
Town hall meetings like the one in Dutse local government authority (pictured), are one example of how SuNMaP 2 brought communities closer to the decision-making process around malaria prevention and control.
In response to the concerns raised by communities, local stakeholders committed to a number of new campaigns including environmental education workshops, house to house awareness promoting mosquito net use and new awareness campaigns in schools.


Impact of programme closure in this area
Without support from SuNMaP 2, responsibility will need to fall to SMEPs to utilise the mechanisms that have been established by the programme to engage community coalitions and other public platforms around malaria prevention and to support budgetary allocation for the malaria programme.
Key achievement 5
Embedding an evidence-based learning environment in NMEP and SMEPs
Embedding an evidence-based learning enviornment in the NMEP and SMEPs also built on a strong foundation left by the predecessor SuNMaP programme, which established a budget for operations research within the NMEP. This led to improved quality of data over the past decade, while paper-based processes have been phased out and activities transitioned to digital systems.
SuNMaP 2 looked to deepen the capabilities and institutionalise the tools for data-informed decision making at a federal, state and district level. Data Informed Decision Making (DIDM) platforms were established in the six supported states and coordinators were trained on the platform to allow the tracking of the use of evidence for decision making.
Other key achievements in this area include:
- Evidence from surveys and analysis of routine HMIS data informed the development of malaria operational plans (MoPs) both at national level and in the six supported SuNMaP 2 states
- Generation and dissemination of granular data at LGA level to guide micro-stratification of malaria intervention mixes
- Establishment of data control rooms at SMEPs to address data quality issues
- Establishment of an entomological site in Kaduna state
- Supported the revision of the NMEP website, including the development of a knowledge hub where evidence and learnings are shared.
CASE STUDY: Data and surveillance for malaria in Nigeria: Q&A with Oluwatosin Ajibade
As a part of SuNMaP 2, Evidence and Learning Specialist, Oluwatosin Ajibade, completed a secondment at the National Malaria Elimination Programme. He spoke in this Q&A about the importance of strengthening malaria surveillance and improving the sharing of disease-related intelligence to empower decision-makers to make informed and timely choices around interventions.
Impact of programme closure in this area
The NMEP and SMEPs will encounter funding gaps for DIDM platforms in the six supported states and for the entomological surveillance site in Kaduna as SuNMaP 2 was supporting the implementation of these interventions exclusively.
Programme disruptors
This programme summary reflects the successes of SuNMaP 2, despite operating for less than half of its original planned time. While the premature closure of the programme is the most obvious disruptor to its success, the final full year of operation also took place amidst the COVID-19 pandemic.
The impact of COVID-19 on SuNMaP 2
Protecting the world's most vulnerable people has been crucial during the COVID-19 pandemic. The delivery of life-saving health services could not be interrupted however, especially at the community level, if an increase in deaths from other diseases, including malaria, were to be avoided. Early in the pandemic, Malaria Consortium made a commitment to follow WHO guidelines and adapt its programming to continue in the safest way possible.
Like much of the world, parts of SuNMaP 2's operations successfully transitioned online - our offices closed and meetings became virtual. However, for malaria service delivery, where people rely on face-to-face community health services to stay healthy and receive diagnosis and treatment, services had to be maintained and in some cases, changed.
SuNMaP 2's community-facing elements, like those involved in SMC and iCCM delivery, were supported in the procurement of personal protective equipment (PPE) including masks, aprons and hand sanitiser.
In addition to the measures listed above, social behaviour change (SBC) methodologies were integrated into SMC distributions in Jigawa to provide implementers and community members with best practices to take part in these activities as safely as possible. SuNMaP 2 also worked with NMEPs and SMEPs to adapt public health messaging to fit the COVID-19 context. Radio spots and SMS campaigns planned to exclusively deliver anti-malaria messaging were adapted to include COVID-19 prevention best practices.

Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices

Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices


Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
Example of SMS messages developed and sent to health workers and members of the public around malaria and COVID-19 best practices
The premature closure of SuNMaP 2
The UK-aid funded SuNMaP 2 programme officially closed on 31st August 2021, after two years of operation and three years short of its originally planned end date.
As a result of the UK aid budget being cut from 0.7 to 0.5 percent of Gross National Income (GNI) and GNI decreasing overall, in 2021, the UK aid budget was cut by £4.1 billion. This cut meant the end of the UK government's bilateral funding for malaria and as such, SuNMaP 2 was told to cease operation immediately.
While the SuNMaP 2 programme was proactive in engaging with the NMEP to seek mitigations to the closure, the decision by the UK government will severely impact Nigeria, particularly in regard to ongoing health and disease programmes. Nigeria has the largest malaria burden in the world, accounting for 27 percent of global cases and 23 percent of global deaths each year.


